Improving the quality of life and tackling premature mortality for people with a learning disability, autism and epilepsy
Home » Blog » Improving the quality of life and tackling premature mortality for people with a learning disability, autism and epilepsy
NHS Midlands and Lancashire (NHS ML), in partnership with national experts at the University of Plymouth, Cornwall Partnership Foundation Trust, SUDEP Action, and Epilepsy Action, among others have supported NHSE Midlands to spearhead a highly successful regional improvement programme to tackle the pressing issue of premature avoidable death among people with learning disabilities and autism living with epilepsy. Read more about work in this case study.
Why is epilepsy in people with a learning disability, autism or both a priority for health and care systems?
Successive LeDeR reports and national reviews, such as the Clive Treacy Independent Review and Norfolk Safeguarding Review into the deaths of Joanna, Jon and Ben, make an urgent and compelling case for action to tackle premature avoidable death and improve the quality of life for people with learning disability, autism or both who suffer from epilepsy.
Figures are stark – sudden death is estimated to be nearly 24 times more likely for all people with epilepsy than those without. For those with a learning disability, who are significantly more likely to have epilepsy and complex epilepsy, this risk is compounded and estimated to be three times higher. The most recent Annual LeDeR Report identified epilepsy as the most common long-term health condition associated with an earlier age at death.
The impact on health services is considerable. 40 per cent of (avoidable) emergency hospital admissions for people with a learning disability are due to convulsions and epilepsy.
Why is now a critical time to drive improvement in epilepsy?
Health inequality is now clearly prioritised in the NHS long-term plan and operational planning guidance with clear expectations set for local healthcare systems to reduce health inequalities. Funding has been made available through core Integrated Care Boards (ICBs) allocations to support the delivery of system plans and includes an adjustment to weight resources in areas with higher avoidable mortality. £200m of additional funding allocated for health inequalities in 2022/23 is also being made recurrent in 2023/24.
Thanks to LeDeR and other national reviews, we understand the experience of health inequality for people with a learning disability in much greater detail than ever before. All Integrated Care Systems (ICSs) are now actively developing plans to address the causes of premature mortality identified through LeDeR, as required by the national LeDeR Policy and there is a real opportunity to ensure that priorities such as epilepsy are embedded in the mainstream strategies to tackle health inequalities and resourced sustainably.
Why is a systematic whole-system approach to tackling premature mortality for people with a learning disability, autism or both in areas of epilepsy and other big killers needed?
We know there is wide variation in the provision of epilepsy services and support as well as issues in relation to the quality of epilepsy care for people with a learning disability and autism. It is a similar experience for other health conditions such as pneumonia, and cancer.
Last summer, we started to engage with all health and care systems across the Midlands to understand the experience of professionals supporting people with a learning disability, autism and epilepsy. We were overwhelmed by the level of enthusiasm and appetite for improvement in this area. There were some great pockets of integrated working that had evolved across community learning disability and specialist epilepsy services. The challenges faced by both commissioners and providers in trying to meet the need were:
lack of awareness and understanding of local needs
lack of effective strategic commissioning
lack of understanding of what good integrated epilepsy services should look like and where systems were falling short.
Systems partners called for improved system-wide strategic planning and service design for this vulnerable group of citizens
How did NHSE Midlands work with NHS ML and national experts to drive improvement across health and care systems across the Midlands?
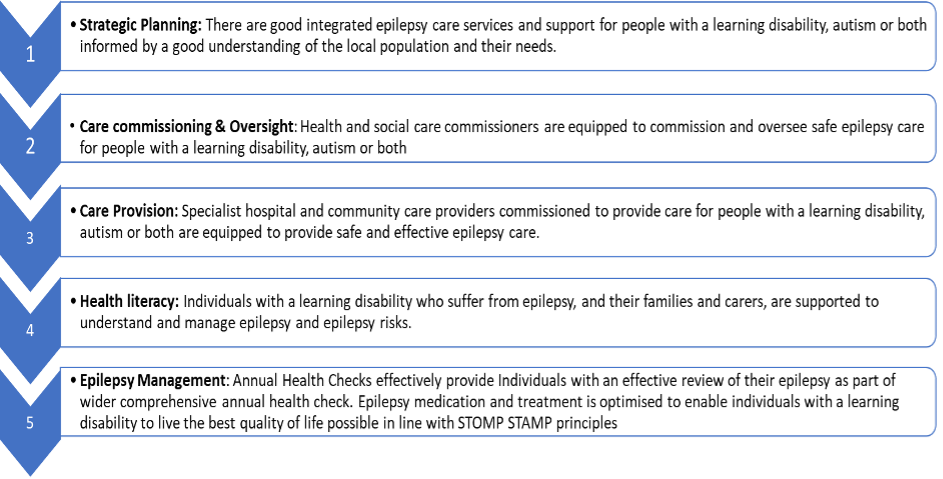
Working with national experts and ICS system leads, NHS ML developed and led the Midlands an LDA Epilepsy Improvement Plan underpinned by five key agreed priorities below.
Putting in place the foundations needed to achieve better outcomes consistently across the Midlands was the priority for 22/23, starting with support for health and care systems to understand their local population and appraise current services, support and pathways.
All Midlands ICSs have been supported to appraise epilepsy services and support using a tailored Learning Disability and Epilepsy Benchmarking Tool developed by Epilepsy Action.
Working through a comprehensive self-assessment questionnaire, this digital tool enables systems to collectively review and benchmark how services and support join together to meet the holistic needs of this population. The tool is based on the Step Together Guidance on Integrated Care for People with a Learning Disability and Autism led by Professor Rohit Shankar of the University of Plymouth and has been developed and tested with four multi-disciplinary teams across the country.
What does the Epilepsy benchmarking exercise involve?
The exercise comprises broadly of three elements as outlined below:
Stage 1: A desktop review with system partners to collate necessary information, input the data and complete the first draft of the self-assessment. A dedicated workshop and drop-in clinics were held to support leads/ champions in coordinating and completing the self-assessment tool.
Stage 2: Consultation: Leads were asked to share the completed first draft self-assessment with all stakeholders to ensure it captures an accurate assessment and submit an updated completed tool to Epilepsy Action for review and analysis.
Stage 3: System-level workshop: ICS leads were asked to bring systems partners together to collectively reflect on the outcome of the self-assessment and develop plans for improvement.
To realise the full benefit of this exercise, we asked ICSs to:
Leadership and Governance: put in place identified senior leads to drive and oversee the delivery of this work including leads with responsibility for neurology/epilepsy services and learning disability and autism services.
Strategic Integration: ensure that this exercise is linked to relevant local strategic programmes relating to epilepsy, learning disability and autism, and health inequalities. Whilst the obvious place for this programme of work might be with learning and disability and autism programmes, it was essential that this exercise also engaged directly with the commissioning and delivery of mainstream epilepsy provision. We suggested that it would be helpful to connect this work with established:
ICS Strategic Health Inequalities Programme
Learning Disability & Autism Programme and LeDeR Programme
Local CYP Epilepsy transformation programme
3. Coordination & delivery: ensure dedicated leads/ champions are identified with the capacity to coordinate this exercise and complete a self-assessment questionnaire. These leads were required to engage with a breadth of system partners to coordinate the tasks outlined in the stages above. Our recommendation was that this role is best supported by a mix of both commissioning and provider champions from LDA and epilepsy disciplines.
4. Stakeholder involvement: engage the full spectrum of system partners who have a role to play in supporting people of all ages with learning disability and epilepsy. It was important that both commissioners and providers worked together to undertake this exercise. Listed below are some key stakeholders we recommended to be involved in the review, but this list is not exhaustive, and we encouraged the system to think widely about who should be engaged.
Patients, families, carers and advocacy groups
Learning disability and autism: NHS and social care LD and autism commissioning leads: community learning disability teams, LD psychiatrists and other clinicians
Epilepsy: Epilepsy/ neurology service commissioning leads, epilepsy nurses, neurologists, epileptologists
Primary care: GPs, primary care liaison nurses
Urgent Care: clinicians and practitioners representing A&E
Social care: Directors of Adult social care/ Social workers and social care practitioners
Learning Disability care and support providers – specialist hospital, residential and supported living providers.
What happens once the benchmarking exercise is completed?
Once completed, the tool creates a system-level report that can be downloaded and shared. System partners have been asked to use this intelligence to guide system-wide reflection and planning of services for people with a learning disability and autism who have epilepsy.
Epilepsy Action prepared and made available a regional report detailing the outcome of all 11 reviews. This provided a helicopter view of epilepsy services and support for people with a learning disability across the Midlands and comparative information for systems on where services and support are advanced and where further attention is needed.
On 31st March 2023, a regional event to share the results of reviews from across the 11 ICSs took place. This provided systems with the space to reflect together on the opportunities for improvement and start the development of improvement plans.
What support was made available to assist ICSs in undertaking this exercise?
Introductory workshop – A dedicated workshop for system leads and partners on how to undertake the review and apply the epilepsy benchmarking tool.
Drop-in advice clinics: These were informal clinics for colleagues to raise any queries or ask for help with any challenges that might arise. They were also an opportunity for colleagues to share progress and learning between systems.
Access to specialist advice: Throughout the process, all systems had access to Professor Rohit Shankar and Epilepsy Action to seek specialist clinical advice and practical advice on how to use the tool.
What tangible outcomes do we expect to see?
Increased focus on improving epilepsy care for people with a learning disability and autism embedded in system-wide improvement to tackle health inequalities
Bringing together system partners across primary, secondary, social care, and voluntary sectors to drive improvement
A shared understanding of the extent to which services are working well together to deliver good care
A shared understanding of where gaps in provision or quality exist, and a springboard for new or enhanced services identified
A shared understanding of workforce capacity & capability, and where further investment is needed
Better use of system-wide resources to improve outcomes.
Foundations in place to support the development of integrated epilepsy care.
Improved integrated strategic commissioning of epilepsy services and support.
We are already seeing tangible outcomes from the work to date across the Midlands including whole system engagement and leadership to drive improvement and targeted investment in specialist epilepsy nurses and other dedicated resources for the LDA population.
How are the wider Midlands LDA Epilepsy Programme priorities being progressed?
Development of practical guidance by SUDEP Action & Cornwall FT for commissioners and care providers (specialist hospital and community) to improve the quality of epilepsy care
Roll out of ‘My Life with Epilepsy Programme, Support & Guidance for Carers’ produced by SUDEP Action
Design of a quality improvement project to pilot a whole system approach to improving the coverage and quality of epilepsy training
Design of a quality improvement project to pilot a PCN approach to strengthening the capability of primary care support working with annual health checks and STOMP/STAMP programmes.
Review of the way in which current pathways engage with assistive technology to manage epilepsy and SUDEP Risk.
What enablers have been critical to the success of the Midlands LDA Epilepsy Improvement Programme?
The input of specialist expertise: The Midlands Epilepsy Advisory Group is a body of national experts and regional leads (including Professor Rohit Shankar of Cornwall FT, Chair of International League Against Epilepsy, SUDEP Action, Epilepsy Action, Epilepsy Nurses Association) that have been invaluable to the programme from the outset
Leadership and engagement of NHSE Midlands and Midlands ICSs
Effective engagement of practitioners across disciplines including, primary, secondary, community and social care
Dedicated programme support to develop and coordinate the improvement programme working closely with the regional team and ICSs.
The national Health and Care Analytics (HACA) Conference returns this December, bringing together analysts, system leaders, and decision-makers from across…
Supporting ICSs with approaches to design and deliver effective communication, engagement and behavioural insights as a key enabler for system change and…
Acting as an independent and trusted partner within the system to facilitate working across stakeholders and integrate elements of the provider system…
Digitising care and partnering with systems for the transformation of digitally enabled service delivery (and other supporting processes) across vision, planning and…
Supporting systems to build a sustainable and integrated workforce, transforming systems, organisations and the workforce experience to improve resilience.
Applying intelligence-led understanding of the health of the population to support the redesign of care and improve patient and financial outcomes across…
Supporting providers to work together at a place and neighbourhood level to manage common resources, integrate community teams, improve health and reduce…