Examining health inequalities among people with learning disabilities in Leicester, Leicestershire, and Rutland
Home » Case studies » Examining health inequalities among people with learning disabilities in Leicester, Leicestershire, and Rutland
This study revealed significant health disparities among people with learning disabilities in Leicester, Leicestershire, and Rutland, prompting targeted prevention efforts, increased awareness of intersectionality, and a focus on admission avoidance for this population.
Background
The Aristotle Xi system, utilised by the Leicester, Leicestershire and Rutland Integrated Care Board (ICB) through NHS Midlands and Lancashire, offers a comprehensive, pseudonymised population-level view of health conditions, demographics, and risk factors. This system aggregates data from various healthcare sources, including GP, hospitals, and prescribing systems. A limited number of practice staff can also access patient-level data. The Public Health Team in Leicestershire County Council conducted an analysis using data from the Aristotle system to investigate the health and health inequalities among people with learning disabilities in the Leicester, Leicestershire, and Rutland (LLR) region.
The primary objectives of this study were:
To examine the health of people with learning disabilities in LLR using data from the Aristotle system
To identify significant differences in the health of people with learning disabilities compared to those without
To explore any health inequalities experienced by people living in areas of high deprivation (the 20% most deprived neighbourhoods according to the Index of Multiple Deprivation).
Action
To achieve these objectives, the following steps were taken.
Identified local population of people with learning disabilities, including their size, age, and sex distribution.
Assessed the proportion of the learning disability population with long-term conditions listed in the Aristotle system, and the proportion at high risk of emergency hospital admission in the next year based on risk stratification tools used in GP practices.
Examined the proportion of the learning disability population residing in the 20% most deprived neighbourhoods and the proportion with each of the long-term conditions living in such neighbourhoods.
Compared the collected data for people with learning disabilities with data from the general population of LLR.
Statistical analysis to determine the significance of any observed differences in proportions.
Impact
The study produced the following key findings.
The registered population of people with learning disabilities across LLR is 4,925.
People with learning disabilities are significantly more likely to live in high-deprivation areas (20% most deprived neighbourhoods) compared to those without learning disabilities.
The learning disability population is four times more likely to be at risk of emergency hospital admission than the general population.
A higher percentage of people with learning disabilities and health conditions live in the 20% most deprived areas compared to those without learning disabilities but with the same health conditions.
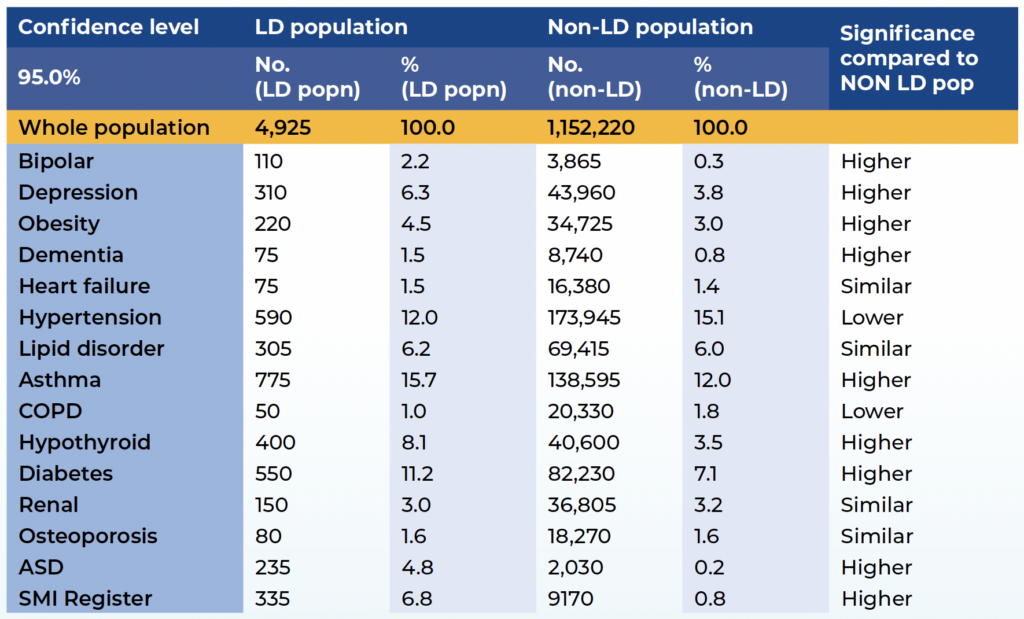
People with learning disabilities are more likely to have health conditions, with a fourfold increase in the likelihood of having five or more chronic conditions compared to those without learning disabilities. Common conditions include asthma, hypertension, and diabetes.
The study identified several health conditions that are significantly more prevalent among people with learning disabilities in the LLR region. The findings are being used to explore targeted prevention opportunities and promote better access and treatment pathways for these conditions among people with learning disabilities.
The higher rates of ill health among those living in the 20% most deprived areas highlight the issue of intersectionality, where individuals experience multiple factors or characteristics that increase the risk of poor health outcomes due to health inequalities. These findings are being disseminated across various forums to address health inequalities in LLR.
Furthermore, the evidence of a higher risk of emergency hospital admission for people with learning disabilities is being incorporated into workstreams focusing on admission avoidance. This suggests that the learning disability population may be a potential area for preventive strategies. This case study underscores the importance of using data-driven insights to address health disparities and improve the healthcare outcomes of vulnerable populations.
Feedback
“Aristotle has finally given us the evidence to prove what we knew anecdotally about the health inequalities faced by people with learning disabilities in our local area. We are using Aristotle to ensure we target the right help in the right place to reduce health inequalities faced by people with learning disabilities in our local area.”
Justin Hammond, Associate Director of Mental Health and Learning Disability, Leicester, Leicestershire and Rutland ICB
Further information
Table 1: Percentage of each population affected by the conditions listed and significance in the learning disability population.
Table 1: Percentage of each population affected by the conditions listed and significance in the learning disability population.
For an accessibility-friendly version of the table, please follow this link: Table 1.
For more information
If you would like to get in touch with us about any of our services, please visit our help and contact page.
The national Health and Care Analytics (HACA) Conference returns this December, bringing together analysts, system leaders, and decision-makers from across…
Supporting ICSs with approaches to design and deliver effective communication, engagement and behavioural insights as a key enabler for system change and…
Acting as an independent and trusted partner within the system to facilitate working across stakeholders and integrate elements of the provider system…
Digitising care and partnering with systems for the transformation of digitally enabled service delivery (and other supporting processes) across vision, planning and…
Supporting systems to build a sustainable and integrated workforce, transforming systems, organisations and the workforce experience to improve resilience.
Applying intelligence-led understanding of the health of the population to support the redesign of care and improve patient and financial outcomes across…
Supporting providers to work together at a place and neighbourhood level to manage common resources, integrate community teams, improve health and reduce…